-
Email info@annnutr.org
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Department of Biochemistry (Laboratory of Pharmacology and Toxicology), Faculty of Science, University of Yaounde 1, Cameroon.
2Agri-Food Safety and One Health Agency (AFS1HA), Cameroon.
*Corresponding author: Wilfred Angie Abia
Department of Biochemistry (Laboratory of Pharmacology and Toxicology), Faculty of Science, University of Yaounde 1,
BP 812, Yaounde, Cameroon.
Email ID: abiawilfred@gmail.com
Received: March 18, 2025
Accepted: Apr 18, 2025
Published Online: Apr 25, 2025
Journal: Annals of Nutrition and Dietetics
Copyright: Abia WA et al. © All rights are reserved Publication Model: Open Access
Citation: Abia WA, Taty BP, Fokwen KE, Djomptchouang HT, Walda IA. Knowledge, awareness, and perception of Cameroonians regarding food contaminants and grain management in relation to cancer. Ann Nutr Diet. 2025; 1(2): 1006.
Food, essential for human health, can ironically become a source of harm when contaminated and or adulterated with harmful substances. This cross-sectional study reports on the awareness, knowledge, and perception of Cameroonians on food carcinogens and cancer. The handling and disposal of visibly spoiled grains that may constitute or serve as risk factors for cancer were examined. A multi-stage (face-to-face, and online) random sampling survey method was used to collect responses from participants using Google Form. Most participants (N=65, 53% females) were holders of master’s (60%) or bachelor’s (30%) degrees, and had good perception of food contamination and food fraud (70%). Some disposed visibly spoiled grains in landfills (29%), while majority throw it around home as feed for uncaged birds (54%) although being aware of the potentially harm to human and animal health (91%). Most participants were familiar with contaminants (76.9%, e.g. aflatoxins) and adulterants (e.g. Sudan dye and formaldehyde, 50%). A majority (89%) were aware of economically motivated adulteration and speculated that such adulterants or unapproved additives are likely to cause harm to consumers’ health (99%). Most participants’ (62%) indicated a family member had once been diagnosed with cancer. Based on cancer victims’ hospital reports (73.8%, diagnosed at terminal stages (31%), some death (6.2%)), breast cancer (61.5%) followed by liver cancer (24.6%) were speculated to be linked to food-intake. From diagnosis to death, majority (52%) of cancer victims lived for up to 2 years, with an estimated 32% that lived for up to 5 years. 80% endorsed the need to encourage and promote awareness raising and sensitization on cancer. Exposure to food carcinogens is a growing food safety and public health concern in Cameroon. Proper information, education, and communication on the prevention, and reduction of natural and or intentionally/illegally added carcinogens in food and associated dietary exposures in Cameroon cannot be over-emphasized.
Keywords: Cancer; Public perceptions; Food contaminants/Adulterants.
Cancer is known to be among the leading causes of death, and its burden continues to increase globally. Some substances present in our foods may be responsible for, or serve as risk factors for cancer [29,33,34]. The International Agency for Research on Cancer (IARC) predicted that the number of new cancer cases globally will rise to 28.4 million in 2040, which is approximately 47% higher when compared to 2020 [36]. Over the last decade, the incidence of lung, liver, breast, and colorectal cancers has increased globally. Lung cancer is the most prevalent type of cancer worldwide [8,28]. Liver cancer is more common in lowand middle-income nations, with parts of Sub-Saharan Africa having significant prevalence [43]. Breast cancer increases with age, with the majority of cases occurring in women over 50 years of age [32]. Colorectal cancer is known to affect both males and women equally, and the risk rises with age [7,31]. Breast and colorectal cancer incidence can also be affected by socioeconomic factors such as income and education level, with higher rates occurring in individuals with a higher socioeconomic standing [27,31]. Lung and liver cancer is more prevalent in men than in women [35].
In Cameroon, the incidence of cancer has been steadily increasing, with 20,745 new cases and 13,199 deaths attributed to cancer in 2020 alone [36,40]. According to WHO’s Global Cancer Observatory (GLOBOCAN), the number of prevalent cases in the last 5 years is 43618 with 19564 and 12789 new cases and deaths respectively [41]. Specifically, GLOBOCAN revealed that liver cancer is Cameroon’s sixth most common cancer, accounting for approximately 4.9% of all new cancer cases. This accounted for approximately 7.2% of all cancer deaths in the country. Also, stomach cancer is the seventh most prevalent cancer in Cameroon, accounting for about 2.3% of all new cancer cases, and ranks as the seventh largest cause of cancer death in Cameroon, accounting for approximately 3.1% of all cancer deaths. Additionally, breast cancer which is the most prevalent cancer among women, was responsible for 4,170 new cases in 2020, accounting for 20.1% of all new cancer cases in the nation. Also, colorectal cancer accounts for 474 new cases in males and 441 in females of all ages in Cameroon. Similarly, lung cancer accounts for approximately 415 of all new cancer cases in Cameroon and is ranked the tenth most prevalent cancer in Cameroon. It also represents the eight largest causes of cancer death in the country, accounting for approximately 3.0% of all cancer deaths. Its prevalence is 1.18 cases per 100,000 people when considering that lung cancer has been on the rise in Cameroon over the last decade, with men being more affected than females [11].
Several factors are known to contribute to the development of cancer such as genetics, lifestyle, environmental factors, and dietary exposure to food carcinogens [29,39]. Natural food contaminants that are carcinogenic include aflatoxins [19,20,24,25], Polycyclic Aromatic Hydrocarbons (PAHs) [24], heavy metals [1,23,24,42], bisphenol A (BPA) [16], and some pesticide residues [7]. Likewise, suspected food adulterants that are classified as carcinogenic include Sudan dye I-V (Group 3 carcinogens, IARC, 1987), formaldehyde/formol (Group 1 carcinogen, [25]), and lead chromate (group 1B, [25]). Preliminary reports from Cameroon on dietary exposures to natural food contaminants include aflatoxins [4-6,37] Njume 2013 and heavy metals such as lead [38]. Additionally, carcinogenic food adulterants such as Sudan dye have been suspected in red palm oil [13]. Notwithstanding, many common food-related contaminants in our diets may be carcinogenic, and may already be known, or not yet known, by consumer populations in Cameroon. Therefore, this cross-sectional study has reported on the awareness, knowledge, and perception of Cameroonians on food carcinogens and cancer, as well as on the handling and disposal of visibly spoiled grains that may constitute or serve as risk factors for cancer.
Study area and approach
The cross-sectional survey was conducted in Cameroon both online and face-to-face between April 2023 and May 2023. A multi-stage random sampling method was followed for sampling respondents. In the first stage, respondents were randomly contacted face-to-face from diversified focussed groups such as “njangi groups”, “food-related business people”, farmers, etc. In the second stage, respondents were randomly contacted online from amongst the over 200 people and groups on various WhatsApp platforms where the authors are members. At the third stage, those whom we contacted, randomly contacted individuals and groups on their various WhatsApp contact lists. These stages were done to get responses from various individuals concerning their knowledge and awareness of cancer, in an unbiased manner.
Participants were Cameroonians from diversified sub-populations stated above, who took an interest in the study and voluntarily dedicated time to respond to the questionnaire. Although ethics approval was not sought for this study, the survey indicated that responding to the questions implies consenting to participate, in which case the prospective participant may seek further information about the study if need be before responding.
Analytical framework
A research instrument consisting of a semi-structured interview/questionnaire was designed. It was done in English and translated into French, taking care not to lose any information for data collection. The semi-structured questionnaire was focused on Cameroonian’s perceptions, knowledge, attitudes, practices, and concerns towards agri-food fraud intra-/and inter-Cameroon trade borders e.g. with the European Union. This questionnaire was later uploaded to Google Form. A Google form link to access the Google form and complete the questionnaire was generated. The data were collected face-to-face (in the form of interviews or questions and answers, with proposed answer choices) of the respondents in stage one. For stage two, the interview questions were placed online as a semi-structured questionnaire using Google Form, and the link was shared with over 200 people and groups on our WhatsApp. At the third stage, those who responded were encouraged to in turn share the questionnaires with those (individuals and groups) on their WhatsApp contact list.
Variables including age, education, occupation, and marital status were assessed and employed in the characterization of the socio-demographic backgrounds of participants. For perceptions, knowledge, attitudes, and practices, suitable statements were developed and validated by the field survey data. The respondents were asked to indicate (Yes, No, or I don’t know) the statement that better described their perception.
Each dataset from the face-to-face (in the form of an interview) of the respondents in stage one was entered into the questionnaire through the Google Form link. Data from all the respondents across stages 1, 2, and 3 were directly merged and analyzed online by the Google Form tool. Descriptive statistics, such as frequencies and percentages were calculated directly by the Google Form tool, and the results were expressed in Tables or charts.
Overall, the online survey questionnaire received responses from a total of 65 Cameroonian participants (the majority were 20-45 years old, 92%), with 53% identifying as female and 46.2% as male. In terms of educational attainment, 60% of the participants held a master’s degree, while 30.8% held a bachelor’s degree, 7.7% held an advanced level certificate, and 1.5% held an ordinary level certificate. With regards to marital status, 60% of the participants were single, 36.9% were married, 1.5% were single parents, and 1% were divorced.
Perception and knowledge of cancer
In terms of participants’ perception and knowledge on cancer (Table 1), the survey results showed that a notable proportion of the participants (13.6%) had never heard of cancer, with only 29.2% of those who were aware of cancer having ever attended a meeting e.g., a seminar on cancer. The majority (70%) had a good perception of food contamination and food fraud, and over 54% were not aware that cancer is a terminal disease. Over 80% of the participants were aware that food sold to them could have been tampered with, and the overall reason for the fraud was to increase economic gains (95%). 98.5% of participants revealed that unapproved additions or adulterations of foods were likely to cause harm to consumers’ health. 76.9% of respondents and more than 50% of the participants claimed to be aware of some carcinogenic contaminants (specifically aflatoxins), and adulterants (e.g. Sudan dye and formaldehyde) in foods.
| Response (%) | |||
|---|---|---|---|
| Yes | No | I don’t know | |
| Have you ever heard of cancer? | 86.4 | 13.6 | 0 |
| Do you know (or have heard) of anyone suffering from cancer? | 81.5 | 16.9 | 0 |
| Is cancer not as common as malaria in Cameroon? | 75.4 | 16.9 | 7.7 |
| Have you ever attended a seminar on cancer? | 29.2 | 70.8 | 0 |
| Do you know (or have heard of) anyone who dies from cancer? | 86.4 | 13.6 | 0 |
| Would you prefer to suffer from cancer instead of any other diseases common in Cameroon like malaria? | 89.2 | 4.6 | 6.2 |
| Is cancer a terminal disease (i.e. you will soon die when you have cancer)? | 44.6 | 44.6 | 10.8 |
| Have you ever heard about food contaminants? | 96.9 | 3.1 | 0 |
| Food contamination is when someone deliberately includes a harmful substance in foods that go to the market. | 35.4 | 59.9 | 7.7 |
| Food contaminants can harm animals and man when we eat them in our feed or food respectively. | 95.4 | 1.5 | 3.1 |
| I have heard that some harmful substances sometimes contaminate our foods and may either serve as risk factors for cancer or can give us cancer when we eat such foods. | 76.9 | 6.2 | 16.9 |
| I have heard of Aflatoxins as one of the harmful substances that sometimes contaminate our foods and may either serve as risk factors for cancer or can give us cancer when we eat such foods. | 76.9 | 10.8 | 12.3 |
| Some agricultural/food commodities in Cameroon such as maize and groundnuts have been reported to contain cancer risk factors. | 64.6 | 10.8 | 24.6 |
| There are no regulations in Cameroon against Aflatoxins levels in some agricultural/food commodities such as maize and groundnuts. | 41.5 | 10.8 | 47.7 |
| I have heard of food fraud. | 89.2 | 9.2 | 1.5 |
| Those who deliberately tamper with food quality before selling it to the public do so to increase their profits. | 95.4 | 1.5 | 3.1 |
| Increasing the profit you make from selling a product through the deliberate addition/mixing of unauthorized or unapproved substances is a bad practice and must not be done. | 95.4 | 1.5 | 3.1 |
| Some of the unauthorized or unapproved substances deliberately included in food may cause harm to our bodies when we consume such foods especially continuously eating them over a long time. | 98.5 | 0 | 1.5 |
| I have heard of Sudan dye as one of the harmful substances that sometimes contaminate our foods and may either serve as risk factors for cancer or can give us cancer when we eat such foods. | 53.8 | 15.4 | 30.8 |
| I have heard of formaldehyde/formalin as one of the harmful substances that sometimes contaminate our foods and may either serve as risk factors for cancer or can give us cancer when we eat such foods. | 76.9 | 7.7 | 15.4 |
| Responses in % | ||||
|---|---|---|---|---|
| Yes | No | It depends | I don't know | |
| Are grains generally hand-picked and or sieved visibly spoiled grains just before preparing/cooking them? | 67.7 | 3.1 | 26.2 | 3.1 |
| Visibly spoiled grains are not good for human health, so should not be eaten by humans. | 90.8 | 3.1 | 3.1 | 3.1 |
| Visibly spoiled grains are good for animal health, so should be given to animals. | 9.2 | 72.3 | 13.8 | 4.6 |
| Has any member of your family (or anyone you know) ever been diagnosed with cancer? | 61.5 | 36.9 | 0 | 1.5 |
| Is/Was s/he placing on regular physical exercises (or Is/Was s/he doing regular physical exercises)? | 21.5 | 30.8 | 0 | 47.7 |
| Is/Was she/he feeding from the same pot with other family members (or Is/Was she/he being cooked separate meals)? | 44.6 | 13.8 | 0 | 41.5 |
| Is/Was the situation of the victim traumatizing to you/or your family members? | 61.5 | 6.2 | 0 | 32.3 |
Grains handling and cancer victims’ management
Table 2 provides data on the handling of grains and local management of cancer victims in Cameroon. The majority (90.8%) of the participants were aware that visibly spoiled grains are not good for human health while 9.2% thought that visibly spoiled grains are good for animal health. 61.5% of participants indicated a family member had once been diagnosed with cancer, which traumatized the family while only 21.5% of those victims did physical exercises.
Awareness of food fraud and disposal of visibly spoiled grains
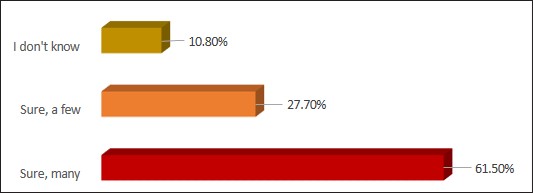
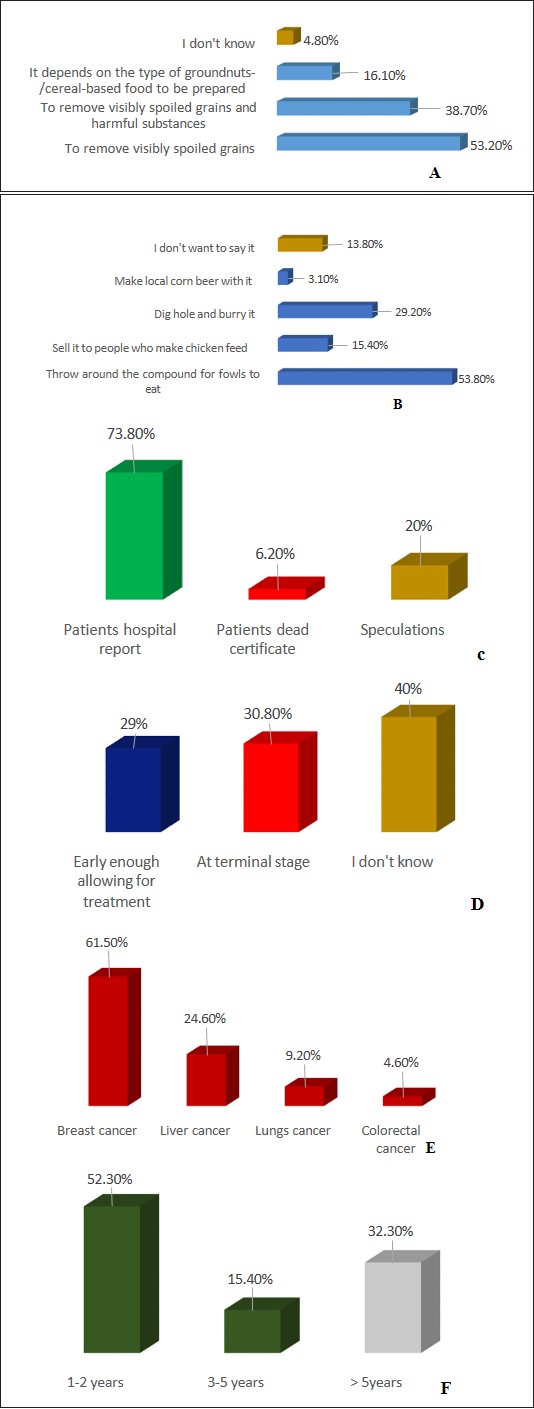
Over 89% of the studied participants revealed that a variety of food products were being manipulated for economic gains (Figure 1). While 53% of respondents revealed they hand sorted visibly spoiled grains and washed grains before processing, 38.7% of them were aware that such a step also removed harmful substances (food contaminants) (Figure 2a). In view of disposal of visibly spoiled grains, although an estimated 14% reserved their opinions; approximately 54% of respondents stated that they usually throw visibly spoiled grains around their homes for uncaged birds to feed on; 29% did landfill; 15% sold visibly spoiled grains to be included in caged birds feed processing; and 3% used visibly spoiled grains to prepare corn beer locally for human consumption (Figure 2b). Based on cancer victims’ hospital reports (73.8%), death reports (6.2%) and speculations (20%) (Figure 2c), participants revealed awareness of cases of diet-related cancer with breast cancer (61.5%) followed by liver cancer (24.6%) as the most cited (Figure 2d). Generally, an estimated 31% of cancer cases were diagnosed at the terminal stage, with 29% diagnosed early enough and allowed for treatment (Figure 2e). From diagnosis to death, a majority (52%) of cancer victims lived for up to 2 years, with an estimated 32% that lived for up to 5 years (Figure 2f).
| Responses in % | |||
|---|---|---|---|
| Agreed fully | Disagreed partially | I don’t know | |
| Encourage and promote awareness raising and sensitization on cancer signs and symptoms at all levels. | 90.8 | 6.2 | 3.1 |
| Encourage and promote consultation by everyone immediately they notice or feel any cancer sign or symptom. | 95.4 | 3.1 | 1.5 |
| Encourage and promote awareness raising and sensitization on cancer risk factors in our diets at all levels | 96.9 | 1.5 | 1.5 |
| Promote the consumption of adequate amounts of a variety of balanced diets. | 98.5 | 1.5 | |
| Encourage routine check-ups for cancer | 89.2 | 7.7 | 3.1 |
| Encourage physical exercise for cancer victims | 83.1 | 9.2 | 7.7 |
Approaches to reduce cancer exposures and or manage victims.
Some proposed strategies to fight against cancer and management of victims are presented in Table 3. The majority (>80%) of respondents endorsed the need to encourage and promote awareness raising and sensitization on cancer. This involved, cancer signs/symptoms, and potential cancer risk factors in diets/foods; routine check-ups of cancer; consultation of a medical practitioner in case any cancer-related sign/symptom is suspected; intakes of a variety of foods and fruits in a balanced diet way; and regular physical exercises for victims.
Food is a complex mixture of chemicals including water, carbohydrates, proteins, and lipids. Certain unavoidable contaminants in foods, such as pesticide residues and aflatoxins may be carcinogenic in acute and or chronic exposures. Such contaminants are either not permitted in foods e.g. aflatoxins B1 [19], or are generally permitted in foods by regulatory bodies at levels considered the lowest level attainable without resulting in severe economic losses, adverse effects on the food supply, or adverse health implications.
Dietary carcinogens (herein interchangeably used with food carcinogens) are substances present in food that have the potential to serve as risk factors for cancer or maybe cancer causing [30]. Although a variety of food contaminants exist [26], this study focused on the naturally occurring food contaminants and those intentionally/illegally added as food adulterants. Meanwhile, some toxigenic microorganisms and plants commonly contaminate foods and produce natural food contaminants during growth, harvest, storage, or processing, food adulterants are tenaciously added to food for economic gains referred to as food fraud [2,14]. Therefore, given the upsurge of cancer in Cameroon in the recent past [41], this cross-sectional study was designed to investigate the awareness, knowledge, and perception of Cameroonians on food carcinogens and cancer. Additionally, it focused on the handling and disposal of visibly spoiled grains generally assumed to be contaminated with mycotoxins such as aflatoxins, and that may constitute or serve as risk factors for cancer.
With the aid of a multi-stage face-to-face and online survey, information was gathered, analyzed, and interpreted as presented in this paper. The findings provide a comprehensive overview of the awareness, knowledge, and perception of Cameroonians regarding dietary carcinogens and cancer incidence in Cameroon. The findings showed that although the majority (86%) of the participants had some knowledge of cancer, while many (71%) of the participants had never had exposure to cancer-related seminars (i.e. no proper information, education, and communication on cancer). This result is consistent with previous studies in low and middle-income countries that revealed a lack of public awareness of cancer and its risk factors [12,22].
Additionally, food contaminants such as aflatoxins were not strange to many participants (77%). This is not only a pointer that aflatoxins are amongst the country’s most important food contaminants of public health concern, but a humble indication of overdue legislation for aflatoxins in Cameroon. For contaminant-specific food legislation to be in place, partly, there is a new for stakeholders’ collaboration. To this end, researchers are encouraged to generate substantial occurrence and dietary exposure data on various carcinogenic food contaminants such as aflatoxins. The government may consider instituting appropriate legislation for selected carcinogenic food contaminants such as aflatoxins. A lot may be learned from the management approach to the cases of aflatoxicosis that occurred in Kenya in 2004 [9] and repeated in 2005 [10] where food and health focused civil society groups, particularly the non-governmental organizations/associations, contributed in addressing the situation via awareness raising. Likewise, the initiative of food and health risk assessment workshops routinely dispensed by the Integrated Health for All Foundation (IHAF) Cameroon may be adopted as part of the approach to addressing food contaminants and adulterants occurrences in foods and associated exposures in Cameroon [3]. In brief, food and health-focused NGOs/Associations may be encouraged to raise awareness via food campaigns to sensitize populations at all levels for a united action against natural and or intentional food contamination. Such efforts may lead individuals and communities to take necessary measures to control and or avoid contamination of their foods, avoid food fraud (adulteration or any other form of tampering with food) with consequential zero or reduced dietary exposures, thus protecting consumers’ health [3]. Such initiatives add substantial contributions towards achieving SDG 3.D (SDG3.D: improve early warning systems for global health risks.) in Cameroon.
Furthermore, most of the participants (>90%) were aware that spoiled grains are unhealthy for both animals and humans. Notwithstanding, spoiled grains are generally used to feed animals. Generally, visibly (and in some cases non-visibly) spoiled grains may be contaminated with carcinogenic aflatoxins amongst other mycotoxins. Aflatoxins is one of the five mycotoxins (aflatoxins, ochratoxins, fumonisins, trichothecenes [deoxynivalenol, nivalenol], and zearalenone) currently recognized as economic and public health concerns [19,20]. Aflatoxins frequently contaminate agricultural commodities such as groundnuts, maize, and their food by-products, generally consumed as staple foods for many in Cameroon [4,37], and aflatoxins B1 is classified as Group 1 carcinogens by the International Agency for Research on Cancer [24,25]. Considering aflatoxins are not easily destroyed by normal cooking temperatures [24,25], feeding animals with spoiled grains and later eating these animals as human food is simply recycling the aflatoxins. It is vital to raise public awareness and understanding of this poor practice of handling spoiled grains. Landfill, practiced by 29% of participants in this present study should be encouraged as a proper disposal approach to visibly spoiled grains [3].
Unlike natural food contaminants, adulterants are intentionally and illegally included in foods. In some cases, the individuals/businesses adding the adulterant may not be aware of its toxic effects on consumers’ health and sometimes on their health as they may even be orally/occupationally exposed to it [3]. Expectedly, food adulteration, a type of food fraud, was not strange to the respondents (89%). Specifically, participants revealed awareness that certain food products in the market may contain intentionally and illegally added adulterants such as formaldehyde (77%) and Sudan dyes (54%). Many participants (95%) denounced such practices perpetrated sorely to increase economic gains, but which are harmful to consumers’ health (99%), and described them as criminal actions (95%). This is in line with the hearsay claims that food fraud may be a serious concern in Cameroon, -although in disarray and pending scientific evidence, and may require urgent attention. For example, Djomptchouang and Abia [13] recently reported that red palm oil sold in markets in Douala and Yaounde in Cameroon is suspicious of Sudan dye adulteration. Food fraud may be commonplace in Cameroon partly due to ignorance, and inadequate monitoring and surveillance of food products put out for consumers, thus allowing business owners to rob consumers’ pockets and jeopardize their almost already poverty-dampened health conditions. Food adulteration is generally perpetrated by food businesses/industries for economic gains [2]. Drivers of adulteration may include but are not limited to, higher demand than production or supply of a food product, absence or inadequate enforcement, of food safety laws, and or inadequate follow-up/feedback from field inspections. Moreover, a calculated network of food adulteration perpetrated by groups of individuals, and or businesses, makes it to become a food crime [15].
The survey results revealed that 45% of the participants believed that cancer is a terminal disease and, thus, may feel discouraged from seeking early diagnosis and treatment. Based on cancer victims’ hospital reports (73.8%) with 31% diagnosed at terminal stages, death due to cancer (6.2%) as well as speculations with no medical reports (20%), participants revealed awareness of cases of diet-related cancer with breast cancer (61.5%) followed by liver cancer (24.6%) as the most cited. This was not strange when considering the report of the Global Burden of Disease (GBD) in 2019 that revealed stomach, breast, esophageal, colorectal, and lung cancers as predominant dietrelated cancers [21] as well as liver cancer [18]. From diagnosis to death, a majority (52%) of cancer victims lived for up to 2 years, with an estimated 32% that lived for up to 5 years. 80% endorsed the need to encourage and promote awareness raising and sensitization on cancer. The findings of this research suggest a need for increased cancer information, education, and communication through awareness campaigns to improve the understanding of cancer among the general population in Cameroon [3]. Such united actions may go a long way towards contributing to the attainment of the sustainable development goal SDG 3.D.
The survey also assessed the participants’ knowledge of the prevention and home management of food-related cancer. The results showed that there is a need for increased education and awareness campaigns to improve the understanding of cancer prevention and home management among the general population. Some approaches rated high by respondents (83-99%), and which may be taken very seriously include encouraging and promoting:
− Awareness raising and sensitization on cancer signs and symptoms, and cancer risk factors in our diets (i.e. carcinogenic food contaminants and adulterants) at all levels,
− Consultation by everyone immediately they notice or feel any cancer signs or symptoms,
− The consumption of adequate amounts of a variety of balanced diets,
− Physical exercise for cancer victims, and
− Routine check-ups for cancer.
It is assumable that 60% of the above-suggested approaches to control and or prevent cancer may be practiced in Cameroon [3]. Dietary carcinogen-related cancers (i.e. cancer induced by carcinogens and or influenced by carcinogenic risk factors) may be managed in Cameroon and thus reverse the situation, thus, reducing diet-related cancer incidence. Therefore, understanding the relationship between food contaminants that may be present in diets in Cameroon and cancer can help guide food safety and public health policies aimed at reducing cancer incidence and burden in Cameroon. The impact of such efforts may contribute towards the national attainment of the sustainable development goal 3, target 3.D.
Altogether, the findings of this study suggest that there is a need for increased education and awareness campaigns to improve the understanding of diet-related cancer inducers and or risk factors. Reducing occurrences in foods, and preventing exposures to carcinogenic food contaminants and or adulterants, as well as home management of cancer victims among the general population are crucial. This requires proper information, education, and communication on food carcinogens to the public.