-
Email info@annnutr.org
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Centre for Food, Food Security and Nutrition Research, Institute of Medical Research and Medicinal Plants Studies, Cameroon.
2Department of Microbiology and Parasitology, University of Buea, Buea, Cameroon.
3Research and Development Department, J&A Oben Foundation, Cameroon
*Corresponding author: Guy Roussel Takuissu
Centre for Food, Food Security and Nutrition Research, Institute of Medical Research and Medicinal Plants Studies, Yaounde, Cameroon.
Email ID: tgroussel@yahoo.fr
Received: Feb 10, 2025
Accepted: Mar 11, 2025
Published Online: Mar 18, 2025
Journal: Annals of Nutrition and Dietetics
Copyright: Takuissu GR et al. © All rights are reserved Publication Model: Open Access
Citation: Takuissu GR, Kenmoe S, Youovop JA, Tchuente BR, Jafarou M, et al. Prevalence of zinc deficiency in type 2 diabetic patients: Systematic review. Ann Nutr Diet. 2025; 1(1): 1002.
Background and aim: Type 2 Diabetes Mellitus (T2DM) is a worldwide health concern that is frequently associated by micronutrient deficiencies, such as zinc. However, the frequency of zinc deficiency in T2DM patients remains little understood. The purpose of this systematic review was to assess the global prevalence of zinc insufficiency among individuals with T2DM.
Methods: We carried out a systematic review following PRISMA principles. We searched Medline, Embase, Global Index Medicus, and Web of Science for studies published in English or French between inception and October 2024, using keywords linked to zinc insufficiency and T2DM. We considered original research that examined the prevalence of zinc insufficiency in T2DM patients. Two independent reviewers screened publications, extracted data, and assessed the likelihood of bias using a modified Hoy tool.
Results: Of the 7143 articles identified, 5 cross-sectional studies involving 492 T2DM patients met our inclusion criteria. The studies were predominantly from the Eastern Mediterranean Region (4/5) and were published between 2005 and 2020. The prevalence of zinc insufficiency, measured by the studies’ criteria employing atomic absorption spectrometry, was 51.21% (252/492). The majority of studies (4/5) showed a moderate risk of bias. Conclusion: This systematic review indicates a high frequency of zinc insufficiency among T2DM patients, notably in the Eastern Mediterranean Region. These findings highlight the importance of increasing zinc status awareness in this population.
Keywords: Type 2 diabetes mellitus; Zinc deficiency; Prevalence; Systematic review.
Type 2 Diabetes Mellitus (T2DM) is a major public health problem that affects millions of people worldwide and places a significant burden on health systems, particularly in Low-and Middle-Income Countries (LMICs) [1,2]. The global prevalence of T2DM has reached alarming levels, with the number of adults affected by the disease estimated to be 463 million in 2019 [1]. T2DM is characterized by chronic hyperglycemia resulting from insulin resistance and beta cell dysfunction [3]. Alongside these metabolic disorders, micronutrient deficiencies, including zinc, are common but often under-recognized [4].
Zinc deficiency affects approximately 17.3% of the global population and remains a widespread nutritional problem [5]. Zinc is an essential trace element involved in many biological processes, including the synthesis, storage, secretion, and action of insulin [6]. It also plays an important role in antioxidant defense mechanisms and immune function, which are often impaired in patients with T2DM [7,8]. In these patients, zinc affects both the structural integrity and function of insulin producing beta cells [9]. Zinc deficiency can exacerbate insulin resistance and oxidative stress, leading to poor glycemic control [10]. Conversely, T2DM affects zinc metabolism and may increase zinc excretion, leading to subsequent deficiency [11]. Despite its importance, zinc deficiency is poorly characterized in T2DM populations, especially in LMICs where dietary deficiencies are common [12].
The prevalence of T2DM is increasing due to urbanization, dietary and lifestyle changes [2]. At the same time, dietary inadequacy and limited access to zinc-rich foods have led to widespread zinc deficiency, exacerbating health inequalities [12]. Systematic reviews of micronutrient deficiencies in T2DM have mostly focused on vitamins D, E, and magnesium, with zinc often overlooked [13,14]. However, several systematic reviews and meta-analyses have demonstrated that individuals with T2DM generally exhibit lower serum zinc levels compared to non-diabetic individuals and that zinc supplementation is associated with improvements in glycemic control and lipid profiles. For instance, Jayawardena et al. (2012) and others have reported that zinc supplementation significantly reduced fasting blood glucose and hemoglobin A1c levels in patients with T2DM [15,16].
Despite the growing body of evidence linking zinc status and diabetes outcomes, the prevalence of zinc deficiency in patients with T2DM has not yet been fully investigated. The aim of this systematic review was to synthesize the existing literature and determine the prevalence of zinc deficiency in patients with T2DM worldwide. By integrating data from different populations, we aim to more clearly understand the extent of zinc deficiency in patients with T2DM, thereby informing clinical practice and guiding future research on the potential benefits of zinc supplementation in diabetes management.
Data sources and search strategy
The systematic review adhered to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, as detailed in PRISMA Checklist (Supplementary Table 1) [17]. The search strategy (Supplementary Table 2) was applied to four databases: Medline, Excerpta Medica Database (Embase), Global Index Medicus, and Web of Science. The search terms were related to zinc deficiency and Type 2 Diabetes. The screening was done on all documents related to zinc deficiency on Type 2 Diabetic patients (T2DM). The search encompassed all relevant literature published in English or French, irrespective of geographical origin, from database inception until October 2024. The review process was conducted between November 2024 and February 2025. This study was registered with International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD42025631858.
Inclusion and exclusion criteria
We included studies that met the following criteria: (a) containing data about the prevalence of zinc deficiency among individuals diagnosed with T2DM, (b) original studies, and (c) published in English or French. Editorials, commentaries, brief reports, research news, systematic review, meta-analyses, studies with a sample size equal or below 10, duplicates and studies without abstracts or full texts were excluded.
Data extraction and management
Completing the duplicate removal, a two-stage level of screening was conducted in the review using Rayyan—Intelligent Systematic Review website (https://www.rayyan.ai/ (accessed on 6 November 2024)). Firstly; two independent reviewers screened the titles and abstracts of all the articles. After the preliminary screening, a pre-designed Google data abstraction form was used to extract data from the selected studies. The different data extracted were: name of the first author, year of publication, study period, study design, sampling approach, number of sites, timing of samples collection, country, WHO region, sample size, zinc quantification method, the number of subjects with zinc deficiency, and participant characteristics (mean age, SD). After data extraction, two reviewers screened the data extracted from all included studies, to enhance accuracy and minimize bias.
Quality assessment
The methodological quality and risk of bias of the included studies, we appraised using the tool developed by Hoy et al. [18] for prevalence studies (Supplementary Table 1). In this scale, two domains were assessed: internal (target population representation, sampling representation, random selection method, and data source) and external (appropriate inclusion criteria, size adequacy, reliability and validity, mode of sample collection, length of study period, reporting numerator(s) and denominator(s) for zinc deficiency prevalence) validity for a total score of 10 points. Each study was assigned a cumulative score out of a maximum of 10 points. Based on the total score, studies were categorized as having a low (7-10 points), moderate (3-6 points), or high (0-3 points) risk of bias (Supplementary Table 1).
Results of literature search
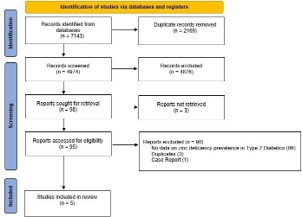
The initial search identified 7143 articles, and 2169 duplicates were excluded (Figure 1). Based on the titles and abstracts, 4876 articles were excluded. The full-text screening of the remaining 98 articles resulted in the exclusion of 93 studies. Finally, 5 articles met our inclusion criteria and were included in the qualitative synthesis.
Characteristics of included studies
The characteristics of included studies are shown in Supplementary (Table 2). All the articles included in this review were cross-sectional and prospectively studies. Articles were published between 2005 and 2020. Study participants ranged in mean age from 45.6 to 57.9 years, and all were recruited from hospital and urban areas (data on study setting didn’t report in one study). The male proportion ranged from 0.00 to 0.53 (data didn’t report in one study). According to the WHO Region, most studies were conducted in Eastern Mediterranean Region (4/5), and one study in Western Pacific. Two studies were conducted in Iran and the 3 other studies in Saudi Arabia, Qatar and China. All the studies used Atomic absorption spectrometry as zinc quantification method. Most of the studies have a moderate risk of bias (4/5) and only one study have a high risk of bias (Supplementary Table 3).
Prevalence of zinc deficiency in type 2 diabetic patients
The 5 included studies reported a total of 492 Type 2 Diabetic patients, of these, 252 were identified as having zinc deficiency, corresponding to a prevalence of 51.21% (Supplementary Table 2).
This systematic review focused on establishing the prevalence of zinc deficiency among patients with T2DM globally. Our findings, based on five studies covering 492 T2DM patients, indicate a pooled prevalence of zinc deficiency of 51.21%. That underpins a substantial comorbidity in this patient cohort which is seldom mentioned.
The observed prevalence is much higher than the approximate global prevalence of zinc deficiency which stands at 17% of the population [5]. This indicates the disproportionate risk of zinc deficiency in T2DM patients. Several factors likely account for this increased risk. The first one is the impairment of zinc absorption and the increase of urinary zinc excretion brought about by chronic hyperglycemia which features T2DM [11,19]. Secondly, low-grade inflammation coupled with T2DM could also affect zinc balance [20]. Thirdly, dietary intake may be deficient; this may be the case in LMIC patients and such patients are likely to have worsened zinc deficiency [12].
Our results agree with previous studies which found that patients with T2DM have lower serum zinc levels in comparison to non-diabetic controls [15,21]. This can be explained by the physiological involvement of zinc in glucose-related metabolism processes. Zinc is essential for the synthesis, storage, and secretion of insulin and for the action of insulin at the cellular [6,9]. Therefore, insulin sensitivity may decline in such individuals and this may worsen glycaemic control evidenced by several interventional studies [15,16].
Nonetheless, it is also wise to point out the limitations of our review. Its small number of studies (n=5) and dominant publication bias limited mainly to the Eastern Mediterranean Region restrained the generalizability of our findings. The observed prevalence might also have been affected by heterogeneity of the study population such as age, duration of the disease and treatments. In addition, all the studies included in this review were only cross-sectional and no claims could be made about possible causality. Another limitation is the reliance on serum zinc levels as the sole indicator of zinc status. Serum zinc is the most commonly used biomarker, but it does not always accurately reflect intracellular zinc levels or overall zinc status, especially in the presence of inflammation [22].
However, our review was not free of those limitations either and we consider that it gives an indication about the proportion zinc deficiency as well among patients living with T2DM. The high burden of disease we documented may warrant greater attention to checking zinc status in this population from the health perspective. Since the prevalence of zinc deficiency in diabetic subjects is high, especially those with poor glycemic control or having a long duration of diabetes and low dietary intake, screening for zinc deficiency should be considered as a routine.
Future research should focus on conducting large-scale, well-designed studies in various regions of the world to estimate zinc deficiency prevalence and determinants among T2DM patients. Longitudinal studies are required to clarify the directional association between zinc deficiency and diabetes outcomes. Our findings have major implications for clinical practice. Addressing zinc deficiency may improve glycemic control, reduce the risk of diabetes-related complications, and improve the overall wellbeing of people with T2DM.
In conclusion, our systematic review indicates a high prevalence of zinc deficiency among individuals with T2DM. This finding warrants further investigation and emphasizes the importance of increasing clinical attention to zinc status in this vulnerable population. Addressing zinc deficiency could provide a new path for improving diabetes care and lowering the global burden of T2DM.
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-forprofit sectors.
Competing interests: The authors have declared that no competing interests exist.
Author contributions: Conceptualization: Guy Roussel Takuissu. Data curation: Sebastien Kenmoe, Guy Roussel Takuissu, Janvier Aimé Youovop, Boris Ronald Tchuente, Mounpou Jafarou. Formal analysis: Sebastien Kenmoe. Methodology: Sebastien Kenmoe, Guy Roussel Takuissu, Janvier Aimé Youovop, Boris Ronald Tchuente, Mounpou Jafarou, Souriou Soufianou. Formal analysis: Sebastien Kenmoe. Project administration: Sebastien Kenmoe, Guy Roussel Takuissu. Supervision: Guy Roussel Takuissu, Gabriel Nama Medoua. Validation: Sebastien Kenmoe, Guy Roussel Takuissu, Janvier Aimé Youovop, Boris Ronald Tchuente, Mounpou Jafarou, Souriou Soufianou, Gabriel Nama Medoua. Writing – original draft: Guy Roussel Takuissu. Writing – review & editing: Sebastien Kenmoe, Guy Roussel Takuissu, Janvier Aimé Youovop, Boris Ronald Tchuente, Mounpou Jafarou, Souriou Soufianou, Gabriel Nama Medoua.
Prisma 2020 checklist statement: The authors have read the PRISMA 2020 Checklist, and the manuscript was prepared and revised according to the PRISMA 2020 Checklist.
| Hoy et al. tool for cross sectional studies | Yes (1)/No (0) |
|---|---|
| 1. Was the study’s target population a close representation of the national population in relation to zinc deficiency prevalence? | 1 |
| 2. Was the sampling frame a true or close representation of the target population? | 1 |
| 3. Was some form of random selection used to select the sample, OR was a census undertaken? | 1 |
| 4. Were data collected directly from the subjects (as opposed to a proxy)? | 1 |
| 5. Was an acceptable inclusion criteria definition used in the study? | 1 |
| 6. Did the author calculate and respect the expected sample size? | 1 |
| 7. Was the zinc quantification assay shown to have reliability and validity? | 1 |
| 8. Was the same mode of data collection used for all subjects? | 1 |
| 9. Was the length of the study period > or = 1 year? | 1 |
| 10. Were the numerator(s) and denominator(s) for the zinc deficiency data appropriate? | 1 |
| Total score | 10 |
| Interpretation of the risk of bias tool 7-10: Low risk of bias 4-6: Moderate risk of bias 0-3: High risk of bias |
Modified from: [12].
| Author | Year of publication | Study design | Timing of samples collection | Country | Study period | Study setting | Setting | Age range | Age (Mean) | Male (Number; Proportion) | Definition of zinc deficiency: Please copy and paste | Zinc Quantification Method | Zinc Deficiency Cases (n) | Total Sample Size (N) | Zinc Levels (Mean/SD) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Asghari et al. | 2019 | cross-sectional | Prospectively | Iran | NR | hospital-based | Urban | 30-60 | 45.85 | 0.53 | Serum zinc levels below the cut-off of 70 μg/dl | Atomic absorption spectrometry | 32 | 60 | 70,85 μg/dl |
| Dorreh et al. | 2013 | cross-sectional | Prospectively | Qatar | NR | hospital-based | Urban | NR | 48.7 | 0.15 | NR | Atomic absorption spectrometry | 6 | 30 | 97.42/32.36 µg/dl |
| Farooq et al. | 2020 | cross-sectional | Prospectively | Saudi Arabia | Mar/2018 - Sep/2018 | hospital-based | Urban | NR | 50.7 | NR | NR | Atomic absorption spectrometry | 171 | 252 | 9.3/1.6 µg/dL |
| Heidari et al. | 2016 | cross-sectional | Prospectively | Iran | Oct/2015 - Feb/2016 | hospital-based | Urban | At least 30 | 45.65/11.60 | 0.5 | NR | Atomic absorption spectrometry | 34 | 100 | 86.45/7.94 µg/dL |
| Lee JungHee et al. | 2005 | cross-sectional | Prospectively | CHINA | NR | Unclear/ Not reported | Unclear/ Not reported | NR | 57.9 | 0.00 | plasma zinc levels were lower than 76 µg/dl | Atomic absorption spectrometry | 9 | 50 | NR |
| Author | Year of publication | Was the study’s target population a close representation of the national population in relation to zinc deficiency prevalence? | Was the sampling frame a true or close representation of the target population? | Was some form of random selection used to select the sample, OR was acensus undertaken? | Was an acceptable inclusion criteria definition used in the study? | Did the author calculate and respect the expected sample size? | Was the zinc deficiency assay shown to have reliability and validity? | Was the same mode of data collection used for all subjects? | Was the length of the study period > or = 1 year? | Were the numerator(s) and denominator(s) for the zinc prevalence? | Risk of bias |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Asghari et al. | 2019 | No | No | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | 6 |
| Dorreh et al. | 2014 | No | No | No | Yes | Unclear | Yes | Yes | Unclear | Yes | 4 |
| Farooq et al. | 2020 | No | No | No | Yes | Unclear | Yes | Yes | No | Yes | 4 |
| Heidari et al. | 2016 | No | No | No | Yes | Unclear | Yes | Yes | No | Yes | 4 |
| Lee JungHee et al. | 2005 | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Yes | 1 |